Tarceva: Package Insert / Prescribing Info
Package insert / product label
Generic name: erlotinib hydrochloride
Dosage form: tablet
Drug class: EGFR inhibitors
Medically reviewed by Drugs.com. Last updated on Jun 17, 2024.
The Tarceva brand name has been discontinued in the U.S. If generic versions of this product have been approved by the FDA, there may be generic equivalents available.
On This Page
- Indications and Usage
- Dosage and Administration
- Dosage Forms and Strengths
- Contraindications
- Warnings and Precautions
- Adverse Reactions/Side Effects
- Drug Interactions
- Use In Specific Populations
- Overdosage
- Description
- Clinical Pharmacology
- Nonclinical Toxicology
- Clinical Studies
- How Supplied/Storage and Handling
- Patient Counseling Information
Highlights of Prescribing Information
TARCEVA (erlotinib) tablets, for oral use
Initial U.S. Approval: 2004
Recent Major Changes
Indications and Usage for Tarceva
TARCEVA is a kinase inhibitor indicated for:
- •
- The treatment of patients with metastatic non-small cell lung cancer (NSCLC) whose tumors have epidermal growth factor receptor (EGFR) exon 19 deletions or exon 21 (L858R) substitution mutations as detected by an FDA-approved test receiving first-line, maintenance, or second or greater line treatment after progression following at least one prior chemotherapy regimen. (1.1)
- •
- First-line treatment of patients with locally advanced, unresectable or metastatic pancreatic cancer, in combination with gemcitabine. (1.2)
Limitations of Use:
Tarceva Dosage and Administration
Dosage Forms and Strengths
Tablets: 25 mg, 100 mg, and 150 mg (3)
Contraindications
None. (4)
Warnings and Precautions
- •
- Interstitial lung disease (ILD): Occurs in 1.1% of patients. Withhold TARCEVA for acute onset of new or progressive unexplained pulmonary symptoms, such as dyspnea, cough and fever. Discontinue TARCEVA if ILD is diagnosed. (5.1)
- •
- Renal failure: Monitor renal function and electrolytes, particularly in patients at risk of dehydration. Withhold TARCEVA for severe renal toxicity. (5.2)
- •
- Hepatotoxicity: Occurs with or without hepatic impairment, including hepatic failure and hepatorenal syndrome: Monitor periodic liver testing. Withhold or discontinue TARCEVA for severe or worsening liver tests. (5.3)
- •
- Gastrointestinal perforations: Discontinue TARCEVA. (5.4)
- •
- Bullous and exfoliative skin disorders: Discontinue TARCEVA. (5.5)
- •
- Cerebrovascular accident (CVA): The risk of CVA is increased in patients with pancreatic cancer. (5.6)
- •
- Microangiopathic hemolytic anemia (MAHA): The risk of MAHA is increased in patients with pancreatic cancer. (5.7)
- •
- Ocular disorders: Discontinue TARCEVA for corneal perforation, ulceration or persistent severe keratitis. (5.8)
- •
- Hemorrhage in patients taking warfarin: Regularly monitor INR in patients taking warfarin or other coumarin-derivative anticoagulants. (5.9)
- •
- Embryo-fetal toxicity: Can cause fetal harm. Advise females of reproductive potential of the potential risk to the fetus and to use effective contraception. (5.10, 8.1, 8.3)
Adverse Reactions/Side Effects
The most common adverse reactions (≥ 20%) with TARCEVA from a pooled analysis in patients with NSCLC across all approved lines of therapy, with and without EGFR mutations, and in patients with pancreatic cancer were rash, diarrhea, anorexia, fatigue, dyspnea, cough, nausea, and vomiting. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact OSI Pharmaceuticals, LLC, at 1-800-572-1932 or FDA at 1-800-FDA-1088 or http://www.fda.gov/medwatch
Drug Interactions
- •
- CYP3A4 inhibitors or a combined CYP3A4 and CYP1A2 inhibitor increase erlotinib plasma concentrations. Avoid concomitant use. If not possible, reduce TARCEVA dose. (2.4, 7)
- •
- CYP3A4 inducers decrease erlotinib plasma concentrations. Avoid concomitant use. If not possible, increase TARCEVA dose. (2.4, 7)
- •
- Cigarette smoking and CYP1A2 inducers decrease erlotinib plasma concentrations. Avoid concomitant use. If not possible, increase TARCEVA dose. (2.4, 7)
- •
- Drugs that increase gastric pH decrease erlotinib plasma concentrations. For proton pump inhibitors avoid concomitant use if possible. For H-2 receptor antagonists, take TARCEVA 10 hours after H-2 receptor antagonist dosing. For use with antacids, separate dosing by several hours. (2.4, 7)
Use In Specific Populations
Lactation: Do not breastfeed (8.2)
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 10/2016
Full Prescribing Information
1. Indications and Usage for Tarceva
1.1 Non-Small Cell Lung Cancer (NSCLC)
TARCEVA® is indicated for:
• The treatment of patients with metastatic non-small cell lung cancer (NSCLC) whose tumors have epidermal growth factor receptor (EGFR) exon 19 deletions or exon 21 (L858R) substitution mutations as detected by an FDA-approved test receiving first-line, maintenance, or second or greater line treatment after progression following at least one prior chemotherapy regimen [see Clinical Studies (14.1, 14.3)].
Limitations of use:
• Safety and efficacy of TARCEVA have not been established in patients with NSCLC whose tumors have other EGFR mutations [see Clinical Studies (14.1, 14.2)].
• TARCEVA is not recommended for use in combination with platinum-based chemotherapy [see Clinical Studies (14.4)].
1.2 Pancreatic Cancer
TARCEVA in combination with gemcitabine is indicated for the first-line treatment of patients with locally advanced, unresectable or metastatic pancreatic cancer [see Clinical Studies (14.5)].
2. Tarceva Dosage and Administration
2.1 Selection of Patients with Metastatic NSCLC
Select patients for the treatment of metastatic NSCLC with TARCEVA based on the presence of EGFR exon 19 deletions or exon 21 (L858R) substitution mutations in tumor or plasma specimens [See Clinical Studies (14.1, 14.2)]. If these mutations are not detected in a plasma specimen, test tumor tissue if available. Information on FDA-approved tests for the detection of EGFR mutations in NSCLC is available at: http://www.fda.gov/CompanionDiagnostics.
2.2 Recommended Dose – NSCLC
The recommended daily dose of TARCEVA for NSCLC is 150 mg taken on an empty stomach, i.e., at least one hour before or two hours after the ingestion of food. Treatment should continue until disease progression or unacceptable toxicity occurs.
2.3 Recommended Dose – Pancreatic Cancer
The recommended daily dose of TARCEVA for pancreatic cancer is 100 mg taken once daily in combination with gemcitabine. Take TARCEVA on an empty stomach, i.e., at least one hour before or two hours after the ingestion of food. Treatment should continue until disease progression or unacceptable toxicity occurs [see Clinical Studies (14.5)].
2.4 Dose Modifications
|
||
|
Adverse Reactions |
||
|
Pulmonary* |
Interstitial Lung Disease (ILD) |
Discontinue TARCEVA |
|
During diagnostic evaluation for possible ILD |
Withhold TARCEVA† |
|
|
Hepatic* |
Severe hepatic toxicity that does not improve significantly or resolve within three weeks |
Discontinue TARCEVA |
|
In patients with pre-existing hepatic impairment or biliary obstruction for doubling of bilirubin or tripling of transaminases values over baseline |
Withhold TARCEVA† and consider discontinuation |
|
|
In patients without pre-existing hepatic impairment for total bilirubin levels greater than 3 times the upper limit of normal or transaminases greater than 5 times the upper limit of normal |
Withhold TARCEVA† and consider discontinuation |
|
|
Renal* |
For severe (CTCAE grade 3 to 4) renal toxicity |
Withhold TARCEVA† and consider discontinuation |
|
Gastrointestinal* |
Gastrointestinal perforation |
Discontinue TARCEVA |
|
For persistent severe diarrhea not responsive to medical management (e.g., loperamide) |
Withhold TARCEVA† |
|
|
Skin* |
Severe bullous, blistering or exfoliating skin conditions |
Discontinue TARCEVA |
|
For severe rash not responsive to medical management |
Withhold TARCEVA† |
|
|
Ocular* |
Corneal perforation or severe ulceration |
Discontinue TARCEVA |
|
For keratitis of (NCI-CTC version 4.0) grade 3-4 or for grade 2 lasting more than 2 weeks |
Withhold TARCEVA† |
|
|
For acute/worsening ocular disorders such as eye pain |
Withhold TARCEVA† and consider discontinuation |
|
|
Drug Interactions |
||
|
CYP3A4 inhibitors‡ |
If severe reactions occur with concomitant use of strong CYP3A4 inhibitors [such as atazanavir, clarithromycin, indinavir, itraconazole, ketoconazole, nefazodone, nelfinavir, ritonavir, saquinavir, telithromycin, troleandomycin (TAO), voriconazole, or grapefruit or grapefruit juice] or when using concomitantly with an inhibitor of both CYP3A4 and CYP1A2 (e.g., ciprofloxacin) |
Reduce TARCEVA by 50 mg decrements; avoid concomitant use if possible |
|
CYP3A4 inducers‡ |
Concomitant use with CYP3A4 inducers, such as rifampin, rifabutin, rifapentine, phenytoin, carbamazepine, phenobarbital, or St. John’s Wort |
Increase TARCEVA by 50 mg increments at 2-week intervals to a maximum of 450 mg as tolerated. Avoid concomitant use if possible |
|
Concurrent cigarette smoking |
Increase TARCEVA by 50 mg increments at 2-week intervals to a maximum of 300 mg. Immediately reduce the dose of TARCEVA to the recommended dose (150 mg or 100 mg daily) upon cessation of smoking |
|
|
Proton Pump inhibitors |
Separation of doses may not eliminate the interaction since proton pump inhibitors affect the pH of the upper GI tract for an extended period |
Avoid concomitant use if possible |
|
H2-receptor antagonists |
If treatment with an H2-receptor antagonist such as ranitidine is required, separate dosing. |
TARCEVA must be taken 10 hours after the H2-receptor antagonist dosing and at least 2 hours before the next dose of the H2-receptor antagonist |
|
Antacids |
The effect of antacids on erlotinib pharmacokinetics has not been evaluated. |
The antacid dose and the TARCEVA dose should be separated by several hours, if an antacid is necessary |
3. Dosage Forms and Strengths
25 mg tablets: round, biconvex face and straight sides, white film-coated, printed in orange with “T” and “25” on one side and plain on other side.
100 mg tablets: round, biconvex face and straight sides, white film-coated, printed in gray with “T” and “100” on one side and plain on other side.
150 mg tablets: round, biconvex face and straight sides, white film-coated, printed in maroon with “T” and “150” on one side and plain on other side.
5. Warnings and Precautions
5.1 Interstitial Lung Disease (ILD)
Cases of serious ILD, including fatal cases, can occur with TARCEVA treatment. The overall incidence of ILD in approximately 32,000 TARCEVA-treated patients in uncontrolled studies and studies with concurrent chemotherapy was approximately 1.1%. In patients with ILD, the onset of symptoms was between 5 days to more than 9 months (median 39 days) after initiating TARCEVA therapy.
Withhold TARCEVA for acute onset of new or progressive unexplained pulmonary symptoms such as dyspnea, cough, and fever pending diagnostic evaluation. If ILD is confirmed, permanently discontinue TARCEVA [see Dosage and Administration (2.4)].
5.2 Renal Failure
Hepatorenal syndrome, severe acute renal failure including fatal cases, and renal insufficiency can occur with TARCEVA treatment. Renal failure may arise from exacerbation of underlying baseline hepatic impairment or severe dehydration. The pooled incidence of severe renal impairment in the 3 monotherapy lung cancer studies was 0.5% in the TARCEVA arms and 0.8% in the control arms. The incidence of renal impairment in the pancreatic cancer study was 1.4% in the TARCEVA plus gemcitabine arm and 0.4% in the control arm. Withhold TARCEVA in patients developing severe renal impairment until renal toxicity is resolved. Perform periodic monitoring of renal function and serum electrolytes during TARCEVA treatment [see Adverse Reactions (6.1) and Dosage and Administration (2.4)].
5.3 Hepatotoxicity with or without Hepatic Impairment
Hepatic failure and hepatorenal syndrome, including fatal cases, can occur with TARCEVA treatment in patients with normal hepatic function; the risk of hepatic toxicity is increased in patients with baseline hepatic impairment. In clinical studies where patients with moderate to severe hepatic impairment were excluded, the pooled incidence of hepatic failure in the 3 monotherapy lung cancer studies was 0.4% in the TARCEVA arms and 0% in the control arms. The incidence of hepatic failure in the pancreatic cancer study was 0.4% in the TARCEVA plus gemcitabine arm and 0.4% in the control arm. In a pharmacokinetic study in 15 patients with moderate hepatic impairment (Child-Pugh B) associated with significant liver tumor burden, 10 of these 15 patients died within 30 days of the last TARCEVA dose. One patient died from hepatorenal syndrome, 1 patient died from rapidly progressing liver failure and the remaining 8 patients died from progressive disease. Six out of the 10 patients who died had baseline total bilirubin > 3 x ULN.
Perform periodic liver testing (transaminases, bilirubin, and alkaline phosphatase) during treatment with TARCEVA. Increased frequency of monitoring of liver function is required for patients with pre-existing hepatic impairment or biliary obstruction. Withhold TARCEVA in patients without pre-existing hepatic impairment for total bilirubin levels greater than 3 times the upper limit of normal or transaminases greater than 5 times the upper limit of normal. Withhold TARCEVA in patients with pre-existing hepatic impairment or biliary obstruction for doubling of bilirubin or tripling of transaminases values over baseline. Discontinue TARCEVA in patients whose abnormal liver tests meeting the above criteria do not improve significantly or resolve within three weeks [see Dosage and Administration (2.4) and Clinical Pharmacology (12.3)].
5.4 Gastrointestinal Perforation
Gastrointestinal perforation, including fatal cases, can occur with TARCEVA treatment. Patients receiving concomitant anti-angiogenic agents, corticosteroids, NSAIDs, or taxane-based chemotherapy, or who have prior history of peptic ulceration or diverticular disease may be at increased risk of perforation [see Adverse Reactions (6.1, 6.2)]. The pooled incidence of gastrointestinal perforation in the 3 monotherapy lung cancer studies was 0.2% in the TARCEVA arms and 0.1% in the control arms. The incidence of gastrointestinal perforation in the pancreatic cancer study was 0.4% in the TARCEVA plus gemcitabine arm and 0% in the control arm. Permanently discontinue TARCEVA in patients who develop gastrointestinal perforation [see Dosage and Administration (2.4)].
5.5 Bullous and Exfoliative Skin Disorders
Bullous, blistering and exfoliative skin conditions, including cases suggestive of Stevens-Johnson syndrome/toxic epidermal necrolysis, which in some cases were fatal, can occur with TARCEVA treatment [see Adverse Reactions (6.1, 6.2)]. The pooled incidence of bullous and exfoliative skin disorders in the 3 monotherapy lung cancer studies was 1.2% in the TARCEVA arms and 0% in the control arms. The incidence of bullous and exfoliative skin disorders in the pancreatic cancer study was 0.4% in the TARCEVA plus gemcitabine arm and 0% in the control arm. Discontinue TARCEVA treatment if the patient develops severe bullous, blistering or exfoliating conditions [see Dosage and Administration (2.4)].
5.6 Cerebrovascular Accident
In the pancreatic carcinoma trial, seven patients in the TARCEVA/gemcitabine group developed cerebrovascular accidents (incidence: 2.5%). One of these was hemorrhagic and was the only fatal event. In comparison, in the placebo/gemcitabine group there were no cerebrovascular accidents. The pooled incidence of cerebrovascular accident in the 3 monotherapy lung cancer studies was 0.6% in the TARCEVA arms and not higher than that observed in the control arms.
5.7 Microangiopathic Hemolytic Anemia with Thrombocytopenia
The pooled incidence of microangiopathic hemolytic anemia with thrombocytopenia in the 3 monotherapy lung cancer studies was 0% in the TARCEVA arms and 0.1% in the control arms. The incidence of microangiopathic hemolytic anemia with thrombocytopenia in the pancreatic cancer study was 1.4% in the TARCEVA plus gemcitabine arm and 0% in the control arm.
5.8 Ocular Disorders
Decreased tear production, abnormal eyelash growth, keratoconjunctivitis sicca or keratitis can occur with TARCEVA treatment and can lead to corneal perforation or ulceration [see Adverse Reactions (6.1) and (6.2)]. The pooled incidence of ocular disorders in the 3 monotherapy lung cancer studies was 17.8% in the TARCEVA arms and 4% in the control arms. The incidence of ocular disorders in the pancreatic cancer study was 12.8% in the TARCEVA plus gemcitabine arm and 11.4% in the control arm. Interrupt or discontinue TARCEVA therapy if patients present with acute or worsening ocular disorders such as eye pain [see Dosage and Administration (2.4)].
5.9 Hemorrhage in Patients Taking Warfarin
Severe and fatal hemorrhage associated with International Normalized Ratio (INR) elevations can occur when TARCEVA and warfarin are administered concurrently. Regularly monitor prothrombin time and INR during TARCEVA treatment in patients taking warfarin or other coumarin-derivative anticoagulants [see Adverse Reactions (6.1) and Drug Interactions (7)].
5.10 Embryo-fetal Toxicity
Based on animal data and its mechanism of action, TARCEVA can cause fetal harm when administered to a pregnant woman. When given during organogenesis, erlotinib administration resulted in embryo-fetal lethality and abortion in rabbits at exposures approximately 3 times the exposure at the recommended human daily dose of 150 mg. Advise pregnant women of the potential risk to a fetus.
Advise females of reproductive potential to use effective contraception during therapy and for one month after the last dose of TARCEVA [see Use in Specific Populations (8.1) and (8.3), Clinical Pharmacology (12.1)].
6. Adverse Reactions/Side Effects
The following serious adverse reactions, which may include fatalities, are discussed in greater detail in other sections of the labeling:
- •
- Interstitial Lung Disease (ILD) [see Warnings and Precautions (5.1)]
- •
- Renal Failure [see Warnings and Precautions (5.2)]
- •
- Hepatotoxicity with or without Hepatic Impairment [see Warnings and Precautions (5.3)]
- •
- Gastrointestinal Perforation [see Warnings and Precautions (5.4)]
- •
- Bullous and Exfoliative Skin Disorders [see Warnings and Precautions (5.5)]
- •
- Cerebrovascular Accident [see Warnings and Precautions (5.6)]
- •
- Microangiopathic Hemolytic Anemia with Thrombocytopenia [see Warnings and Precautions (5.7)]
- •
- Ocular Disorders [see Warnings and Precautions (5.8)]
- •
- Hemorrhage in Patients Taking Warfarin [see Warnings and Precautions (5.9)]
6.1 Clinical Trial Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Safety evaluation of TARCEVA is based on more than 1200 cancer patients who received TARCEVA as monotherapy, more than 300 patients who received TARCEVA 100 or 150 mg plus gemcitabine, and 1228 patients who received TARCEVA concurrently with other chemotherapies. The most common adverse reactions with TARCEVA are rash and diarrhea usually with onset during the first month of treatment. The incidences of rash and diarrhea from clinical studies of TARCEVA for the treatment of NSCLC and pancreatic cancer were 70% for rash and 42% for diarrhea.
Non-Small Cell Lung Cancer
First-Line Treatment of Patients with EGFR Mutations
The most frequent (≥ 30%) adverse reactions in TARCEVA-treated patients were diarrhea, asthenia, rash, cough, dyspnea, and decreased appetite. In TARCEVA-treated patients the median time to onset of rash was 15 days and the median time to onset of diarrhea was 32 days.
The most frequent Grade 3-4 adverse reactions in TARCEVA-treated patients were rash and diarrhea.
Dose interruptions or reductions due to adverse reactions occurred in 37% of TARCEVA-treated patients, and 14.3% of TARCEVA-treated patients discontinued therapy due to adverse reactions. In TARCEVA-treated patients, the most frequently reported adverse reactions leading to dose modification were rash (13%), diarrhea (10%), and asthenia (3.6%).
Common adverse reactions in Study 1, occurring in at least 10% of patients who received TARCEVA or chemotherapy and an increase in ≥ 5% in the TARCEVA-treated group, are graded by National Cancer Institute Common Toxicity Criteria for Adverse Events version 3.0 (NCI-CTCAE v3.0) Grade in Table 1. The median duration of TARCEVA treatment was 9.6 months in Study 1.
|
||||
|
TARCEVA N = 84 |
Chemotherapy* N = 83 |
|||
|
Adverse Reaction |
All Grades % |
Grades 3-4 % |
All Grades % |
Grades 3-4 % |
|
Rash † |
85 |
14 |
5 |
0 |
|
Diarrhea |
62 |
5 |
21 |
1 |
|
Cough |
48 |
1 |
40 |
0 |
|
Dyspnea |
45 |
8 |
30 |
4 |
|
Dry skin |
21 |
1 |
2 |
0 |
|
Back pain |
19 |
2 |
5 |
0 |
|
Chest pain |
18 |
1 |
12 |
0 |
|
Conjunctivitis |
18 |
0 |
0 |
0 |
|
Mucosal inflammation |
18 |
1 |
6 |
0 |
|
Pruritus |
16 |
0 |
1 |
0 |
|
Paronychia |
14 |
0 |
0 |
0 |
|
Arthralgia |
13 |
1 |
6 |
1 |
|
Musculoskeletal pain |
11 |
1 |
1 |
0 |
Hepatic Toxicity: One TARCEVA-treated patient experienced fatal hepatic failure and four additional patients experienced grade 3-4 liver test abnormalities in Study 1 [see Warnings and Precautions (5.3)].
Maintenance Treatment
Adverse reactions, regardless of causality, that occurred in at least 3% of patients treated with single-agent TARCEVA at 150 mg and at least 3% more often than in the placebo group in the randomized maintenance trial (Study 3) are summarized by NCI-CTCAE v3.0 Grade in Table 2.
The most common adverse reactions in patients receiving single-agent TARCEVA 150 mg were rash and diarrhea. Grade 3-4 rash and diarrhea occurred in 9% and 2%, respectively, in TARCEVA-treated patients. Rash and diarrhea resulted in study discontinuation in 1% and 0.5% of TARCEVA-treated patients, respectively. Dose reduction or interruption for rash and diarrhea was needed in 5% and 3% of patients, respectively. In TARCEVA-treated patients the median time to onset of rash was 10 days, and the median time to onset of diarrhea was 15 days.
|
||||||
|
Adverse Reaction |
TARCEVA N = 433 |
PLACEBO N = 445 |
||||
|
Any Grade |
Grade 3 |
Grade 4 |
Any Grade |
Grade 3 |
Grade 4 |
|
|
% |
% |
% |
% |
% |
% |
|
|
Rash * |
60 |
9 |
0 |
9 |
0 |
0 |
|
Diarrhea |
20 |
2 |
0 |
4 |
0 |
0 |
Liver test abnormalities including ALT elevations were observed at Grade 2 or greater severity in 3% of TARCEVA-treated patients and 1% of placebo-treated patients. Grade 2 and above bilirubin elevations were observed in 5% of TARCEVA-treated patients and in < 1% in the placebo group [see Dosage and Administration (2.4) and Warnings and Precautions (5.3)].
Second/Third Line Treatment
Adverse reactions, regardless of causality, that occurred in at least 10% of patients treated with single-agent TARCEVA at 150 mg and at least 5% more often than in the placebo group in the randomized trial of patients with NSCLC are summarized by NCI-CTC v2.0 Grade in Table 3.
The most common adverse reactions in this patient population were rash and diarrhea. Grade 3-4 rash and diarrhea occurred in 9% and 6%, respectively, in TARCEVA-treated patients. Rash and diarrhea each resulted in study discontinuation in 1% of TARCEVA-treated patients. Six percent and 1% of patients needed dose reduction for rash and diarrhea, respectively. The median time to onset of rash was 8 days, and the median time to onset of diarrhea was 12 days.
|
||||||
|
Adverse Reaction |
TARCEVA 150 mg N=485 |
Placebo N=242 |
||||
|
Any Grade |
Grade 3 |
Grade 4 |
Any Grade |
Grade 3 |
Grade 4 |
|
|
% |
% |
% |
% |
% |
% |
|
|
Rash * |
75 |
8 |
<1 |
17 |
0 |
0 |
|
Diarrhea |
54 |
6 |
<1 |
18 |
<1 |
0 |
|
Anorexia |
52 |
8 |
1 |
38 |
5 |
<1 |
|
Fatigue |
52 |
14 |
4 |
45 |
16 |
4 |
|
Dyspnea |
41 |
17 |
11 |
35 |
15 |
11 |
|
Nausea |
33 |
3 |
0 |
24 |
2 |
0 |
|
Infection |
24 |
4 |
0 |
15 |
2 |
0 |
|
Stomatitis |
17 |
<1 |
0 |
3 |
0 |
0 |
|
Pruritus |
13 |
<1 |
0 |
5 |
0 |
0 |
|
Dry skin |
12 |
0 |
0 |
4 |
0 |
0 |
|
Conjunctivitis |
12 |
<1 |
0 |
2 |
<1 |
0 |
|
Keratoconjunctivitis sicca |
12 |
0 |
0 |
3 |
0 |
0 |
Liver function test abnormalities [including elevated alanine aminotransferase (ALT), aspartate aminotransferase (AST) and bilirubin] were observed in patients receiving single-agent TARCEVA 150 mg. These elevations were mainly transient or associated with liver metastases. Grade 2 [> 2.5 – 5.0 x upper limit of normal (ULN)] ALT elevations occurred in 4% and < 1% of TARCEVA and placebo treated patients, respectively. Grade 3 (> 5.0 – 20.0 x ULN) elevations were not observed in TARCEVA-treated patients. TARCEVA dosing should be interrupted or discontinued if changes in liver function are severe [see Dosage and Administration (2.4)].
Pancreatic Cancer - TARCEVA Administered Concurrently with Gemcitabine
This was a randomized, double-blind, placebo-controlled study of TARCEVA (150 mg or 100 mg daily) or placebo plus gemcitabine (1000 mg/m2 by intravenous infusion) in patients with locally advanced, unresectable or metastatic pancreatic cancer (Study 5). The safety population comprised 282 patients in the erlotinib group (259 in the 100 mg cohort and 23 in the 150 mg cohort) and 280 patients in the placebo group (256 in the 100 mg cohort and 24 in the 150 mg cohort).
Adverse reactions that occurred in at least 10% of patients treated with TARCEVA 100 mg plus gemcitabine in the randomized trial of patients with pancreatic cancer (Study 5) were graded according to NCI-CTC v2.0 in Table 4.
The most common adverse reactions in pancreatic cancer patients receiving TARCEVA 100 mg plus gemcitabine were fatigue, rash, nausea, anorexia and diarrhea. In the TARCEVA plus gemcitabine arm, Grade 3-4 rash and diarrhea were each reported in 5% of patients. The median time to onset of rash and diarrhea was 10 days and 15 days, respectively. Rash and diarrhea each resulted in dose reductions in 2% of patients, and resulted in study discontinuation in up to 1% of patients receiving TARCEVA plus gemcitabine. Severe adverse reactions (≥ Grade 3 NCI-CTC) in the TARCEVA plus gemcitabine group with incidences < 5% included syncope, arrhythmias, ileus, pancreatitis, hemolytic anemia including microangiopathic hemolytic anemia with thrombocytopenia, myocardial infarction/ischemia, cerebrovascular accidents including cerebral hemorrhage, and renal insufficiency [see Warnings and Precautions (5)].
The 150 mg cohort was associated with a higher rate of certain class-specific adverse reactions including rash and required more frequent dose reduction or interruption.
|
||||||
|
Adverse Reaction |
TARCEVA + Gemcitabine
|
Placebo + Gemcitabine
|
||||
|
Any Grade |
Grade 3 |
Grade 4 |
Any Grade |
Grade 3 |
Grade 4 |
|
|
% |
% |
% |
% |
% |
% |
|
|
Rash * |
70 |
5 |
0 |
30 |
1 |
0 |
|
Diarrhea |
48 |
5 |
<1 |
36 |
2 |
0 |
|
Decreased weight |
39 |
2 |
0 |
29 |
<1 |
0 |
|
Infection † |
39 |
13 |
3 |
30 |
9 |
2 |
|
Pyrexia |
36 |
3 |
0 |
30 |
4 |
0 |
|
Stomatitis |
22 |
<1 |
0 |
12 |
0 |
0 |
|
Depression |
19 |
2 |
0 |
14 |
<1 |
0 |
|
Cough |
16 |
0 |
0 |
11 |
0 |
0 |
|
Headache |
15 |
<1 |
0 |
10 |
0 |
0 |
Ten patients (4%) in the TARCEVA/gemcitabine group and three patients (1%) in the placebo/gemcitabine group developed deep venous thrombosis. The overall incidence of grade 3 or 4 thrombotic events, including deep venous thrombosis was 11% for TARCEVA plus gemcitabine and 9% for placebo plus gemcitabine.
The incidences of liver test abnormalities (≥ Grade 2) in Study 5 are provided in Table 5 [see Dosage and Administration (2.4) and Warnings and Precautions (5.3)].
|
TARCEVA + Gemcitabine
|
Placebo + Gemcitabine
|
|||||
|
Grade 2 |
Grade 3 |
Grade 4 |
Grade 2 |
Grade 3 |
Grade 4 |
|
|
Bilirubin |
17% |
10% |
<1% |
11% |
10% |
3% |
|
ALT |
31% |
13% |
<1% |
22% |
9% |
0% |
|
AST |
24% |
10% |
<1% |
19% |
9% |
0% |
NSCLC and Pancreatic Indications: Selected Low Frequency Adverse Reactions
Gastrointestinal Disorders
Cases of gastrointestinal bleeding (including fatalities) have been reported, some associated with concomitant warfarin or NSAID administration [see Warnings and Precautions (5.9) and Drug Interactions (7)]. These adverse reactions were reported as peptic ulcer bleeding (gastritis, gastroduodenal ulcers), hematemesis, hematochezia, melena and hemorrhage from possible colitis.
6.2 Post-Marketing Experience
The following adverse reactions have been identified during post approval use of TARCEVA. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Musculoskeletal and Connective Tissue Disorders: myopathy, including rhabdomyolysis, in combination with statin therapy
Eye Disorders: ocular inflammation including uveitis
7. Drug Interactions
CYP3A4 Inhibitors
Co-administration of TARCEVA with a strong CYP3A4 inhibitor or a combined CYP3A4 and CYP1A2 inhibitor increased erlotinib exposure. Erlotinib is metabolized primarily by CYP3A4 and to a lesser extent by CYP1A2. Increased erlotinib exposure may increase the risk of exposure-related toxicity [see Clinical Pharmacology (12.3)].
Avoid co-administering TARCEVA with strong CYP3A4 inhibitors (e.g., boceprevir, clarithromycin, conivaptan, indinavir, itraconazole, ketoconazole, lopinavir/ritonavir, nefazodone, nelfinavir, posaconazole, ritonavir, saquinavir, telithromycin, voriconazole, grapefruit or grapefruit juice) or a combined CYP3A4 and CYP1A2 inhibitor (e.g., ciprofloxacin). Reduce the TARCEVA dosage when co-administering with a strong CYP3A4 inhibitor or a combined CYP3A4 and CYP1A2 inhibitor if co-administration is unavoidable [see Dosage and Administration (2.4)].
CYP3A4 Inducers
Pre-treatment with a CYP3A4 inducer prior to TARCEVA decreased erlotinib exposure [see Clinical Pharmacology (12.3)]. Increase the TARCEVA dosage if co-administration with CYP3A4 inducers (e.g., carbamazepine, phenytoin, rifampin, rifabutin, rifapentine, phenobarbital and St. John's wort) is unavoidable [see Dosage and Administration (2.4)].
CYP1A2 Inducers and Cigarette Smoking
Cigarette smoking decreased erlotinib exposure. Avoid smoking tobacco (CYP1A2 inducer) and avoid concomitant use of TARCEVA with moderate CYP1A2 inducers (e.g., teriflunomide, rifampin, or phenytoin). Increase the TARCEVA dosage in patients that smoke tobacco or when co-administration with moderate CYP1A2 inducers is unavoidable [see Dosage and Administration (2.4) and Clinical Pharmacology (12.3)].
Drugs the Increase Gastric pH
Co-administration of TARCEVA with proton pump inhibitors (e.g., omeprazole) and H-2 receptor antagonists (e.g., ranitidine) decreased erlotinib exposure [see Clinical Pharmacology (12.3)]. For proton pump inhibitors, avoid concomitant use if possible. For H-2 receptor antagonists and antacids, modify the dosing schedule [see Dosage and Administration (2.4)]. Increasing the dose of TARCEVA when co-administered with gastric PH elevating agents is not likely to compensate for the loss of exposure.
Anticoagulants
Interaction with coumarin-derived anticoagulants, including warfarin, leading to increased International Normalized Ratio (INR) and bleeding adverse reactions, which in some cases were fatal, have been reported in patients receiving TARCEVA. Regularly monitor prothrombin time or INR in patients taking coumarin-derived anticoagulants. Dose modifications of TARCEVA are not recommended [see Warnings and Precautions (5.9) and Adverse Reactions (6.1)].
8. Use In Specific Populations
8.1 Pregnancy
Risk Summary
Based on animal data and its mechanism of action, TARCEVA can cause fetal harm when administered to a pregnant woman. Limited available data on use of TARCEVA in pregnant women are not sufficient to inform a risk of major birth defects or miscarriage. When given during organogenesis, erlotinib administration resulted in embryo-fetal lethality and abortion in rabbits at exposures approximately 3 times the exposure at the recommended human daily dose of 150 mg. Advise pregnant women of the potential risk to a fetus.
In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively.
Data
Animal Data
Erlotinib has been shown to cause maternal toxicity resulting in embryo-fetal lethality and abortion in rabbits when given during the period of organogenesis at doses that result in plasma drug concentrations approximately 3 times those achieved at the recommended dose in humans (AUCs at 150 mg daily dose). During the same period, there was no increase in the incidence of embryo-fetal lethality or abortion in rabbits or rats at doses resulting in exposures approximately equal to those in humans at the recommended daily dose. In an independent fertility study female rats treated with 30 mg/m2/day or 60 mg/m2/day (0.3 or 0.7 times the recommended daily dose, on a mg/m2 basis) of erlotinib had an increase in early resorptions that resulted in a decrease in the number of live fetuses.
No teratogenic effects were observed in rabbits or rats dosed with erlotinib during organogenesis at doses up to 600 mg/m2/day in the rabbit (3 times the plasma drug concentration seen in humans at 150 mg/day) and up to 60 mg/m2/day in the rat (0.7 times the recommended dose of 150 mg/day on a mg/m2 basis).
8.2 Lactation
Risk Summary
There are no data on the presence of erlotinib in human milk, or the effects of erlotinib on the breastfed infant or on milk production. Because of the potential for serious adverse reactions in breastfed infants from TARCEVA, including interstitial lung disease, hepatotoxicity, bullous and exfoliative skin disorders, microangiopathic hemolytic anemia with thrombocytopenia, ocular disorders, and diarrhea. Advise a lactating woman not to breastfeed during treatment with TARCEVA and for 2 weeks after the final dose.
8.3 Females and Males of Reproductive Potential
Contraception
Females
TARCEVA can cause fetal harm when administered to a pregnant woman [see Use in Specific Populations (8.1)]. Advise females of reproductive potential to use effective contraception during treatment with TARCEVA and for one month after the last dose of TARCEVA.
8.4 Pediatric Use
The safety and effectiveness of TARCEVA in pediatric patients have not been established.
In an open-label, multicenter trial, 25 pediatric patients (median age 14 years, range 3-20 years) with recurrent or refractory ependymoma were randomized (1:1) to TARCEVA or etoposide. Thirteen patients received TARCEVA at a dose of 85 mg/m2/day orally until disease progression, death, patient request, investigator decision to discontinue study drug, or intolerable toxicity. Four patients randomized to etoposide also received TARCEVA following disease progression. The trial was terminated prematurely for lack of efficacy; there were no objective responses observed in these 17 TARCEVA-treated patients.
No new adverse events were identified in the pediatric population.
Based on the population pharmacokinetics analysis conducted in 105 pediatric patients (2 to 21 years old) with cancer, the geometric mean estimates of CL/F/BSA (apparent clearance normalized to body surface area) were comparable across the three age groups: 2-6 years (n = 29), 7-16 years (n = 59), and 17-21 years (n = 17).
8.5 Geriatric Use
Of the 1297 subjects in clinical studies of TARCEVA for the treatment of NSCLC and pancreatic cancer 40% were 65 and older while 10% were 75 and older. No overall differences in safety or efficacy were observed between subjects 65 years and older and those younger than 65.
8.6 Hepatic Impairment
Hepatic failure and hepatorenal syndrome, including fatal cases, can occur with TARCEVA treatment in patients with normal hepatic function; the risk of hepatic toxicity is increased in patients with baseline hepatic impairment [see Warnings and Precautions (5.3), Adverse Reactions (6.1, 6.2), and Dosage and Administration]. Monitor patients with hepatic impairment (total bilirubin greater than upper limit of normal (ULN) or Child-Pugh A, B and C) during therapy with TARCEVA. Treatment with TARCEVA should be used with increased monitoring in patients with total bilirubin greater than 3 x ULN [see Warnings and Precautions (5.3), Adverse Reactions (6.1, 6.2), and Dosage and Administration (2.4)].
10. Overdosage
Withhold TARCEVA in patients with an overdose or suspected overdose and institute symptomatic treatment.
11. Tarceva Description
TARCEVA (erlotinib), a kinase inhibitor, is a quinazolinamine with the chemical name N-(3-ethynylphenyl)-6,7-bis(2-methoxyethoxy)-4-quinazolinamine. TARCEVA contains erlotinib as the hydrochloride salt that has the following structural formula:
Erlotinib hydrochloride has the molecular formula C22H23N3O4.HCl and a molecular weight of 429.90. The molecule has a pKa of 5.42 at 25°C. Erlotinib hydrochloride is very slightly soluble in water, slightly soluble in methanol and practically insoluble in acetonitrile, acetone, ethyl acetate and hexane.
Aqueous solubility of erlotinib hydrochloride is dependent on pH with increased solubility at a pH of less than 5 due to protonation of the secondary amine. Over the pH range of 1.4 to 9.6, maximal solubility of approximately 0.4 mg/mL occurs at a pH of approximately 2.
TARCEVA tablets for oral administration are available in three dosage strengths containing erlotinib hydrochloride (27.3 mg, 109.3 mg and 163.9 mg) equivalent to 25 mg, 100 mg and 150 mg erlotinib and the following inactive ingredients: lactose monohydrate, hypromellose, hydroxypropyl cellulose, magnesium stearate, microcrystalline cellulose, sodium starch glycolate, sodium lauryl sulfate and titanium dioxide. The tablets also contain trace amounts of color additives, including FD&C Yellow #6 (25 mg only) for product identification.
12. Tarceva - Clinical Pharmacology
12.1 Mechanism of Action
Epidermal growth factor receptor (EGFR) is expressed on the cell surface of both normal and cancer cells. In some tumor cells signaling through this receptor plays a role in tumor cell survival and proliferation irrespective of EGFR mutation status. Erlotinib reversibly inhibits the kinase activity of EGFR, preventing autophosphorylation of tyrosine residues associated with the receptor and thereby inhibiting further downstream signaling. Erlotinib binding affinity for EGFR exon 19 deletion or exon 21 (L858R) mutations is higher than its affinity for the wild type receptor. Erlotinib inhibition of other tyrosine kinase receptors has not been fully characterized.
12.3 Pharmacokinetics
Absorption
Erlotinib is about 60% absorbed after oral administration. Peak plasma levels occur 4 hours after dosing.
Effect of Food
Food increased the bioavailability of erlotinib to approximately 100%.
Distribution:
Erlotinib is 93% protein bound to plasma albumin and alpha-1 acid glycoprotein (AAG).
Erlotinib has an apparent volume of distribution of 232 liters.
Elimination
Erlotinib is eliminated with a median half-life of 36.2 hours in patients receiving the single-agent TARCEVA 2nd/3rd line regimen. Time to reach steady state plasma concentration would therefore be 7-8 days.
Metabolism
Erlotinib is metabolized primarily by CYP3A4 and to a lesser extent by CYP1A2, and the extrahepatic isoform CYP1A1, in vitro.
Excretion
Following a 100 mg oral dose, 91% of the dose was recovered: 83% in feces (1% of the dose as intact parent) and 8% in urine (0.3% of the dose as intact parent).
Specific Populations
Neither age, body weight, nor gender had a clinically significant effect on the systemic exposure of erlotinib in NSCLC patients receiving single-agent TARCEVA for 2nd/3rd line treatment or for maintenance treatment, and in pancreatic cancer patients who received erlotinib plus gemcitabine. The pharmacokinetics of TARCEVA in patients with compromised renal function is unknown.
Patients with Hepatic Impairment
In vitro and in vivo evidence suggest that erlotinib is cleared primarily by the liver. However, erlotinib exposure was similar in patients with moderately impaired hepatic function (Child-Pugh B) compared with patients with adequate hepatic function including patients with primary liver cancer or hepatic metastases.
Patients That Smoke Tobacco Cigarettes
In a single-dose pharmacokinetics trial in healthy volunteers, cigarette smoking (moderate CYP1A2 inducer) increased erlotinib clearance and decreased erlotinib AUC0-inf by 64% (95% CI, 46-76%) in current smokers compared with former/never smokers. In a NSCLC trial, current smokers achieved erlotinib steady-state trough plasma concentrations which were approximately 2-fold less than the former smokers or patients who had never smoked. This effect was accompanied by a 24% increase in apparent erlotinib plasma clearance. In another study which was conducted in NSCLC patients who were current smokers, pharmacokinetic analyses at steady-state indicated a dose-proportional increase in erlotinib exposure when the TARCEVA dose was increased from 150 mg to 300 mg. [see Dosage and Administration (2.4), Drug Interactions (7) and Patient Counseling Information (17)].
Drug Interaction Studies
Co-administration of gemcitabine had no effect on erlotinib plasma clearance.
CYP3A4 Inhibitors
Co-administration with a strong CYP3A4 inhibitor, ketoconazole, increased erlotinib AUC by 67%. Co-administration with a combined CYP3A4 and CYP1A2 inhibitor, ciprofloxacin, increased erlotinib exposure [AUC] by 39%, and increased erlotinib maximum concentration [Cmax] by 17%. [see Dose Modifications (2.4), Drug Interactions (7)].
CYP3A4 Inducers
Pre-treatment with the CYP3A4 inducer rifampicin, for 7-11 days prior to TARCEVA, decreased erlotinib AUC by 58% to 80% [see Dose Modifications (2.4), Drug Interactions (7)].
CYP1A2 Inducers or Smoking Tobacco
See Specific Populations Section [see Dose Modifications (2.4), Drug Interactions (7)].
Drugs that Increase Gastric pH
Erlotinib solubility is pH dependent and decreases as pH increases. When a proton pump inhibitor (omeprazole) was co-administered with TARCEVA the erlotinib exposure [AUC] was decreased by 46% and the erlotinib maximum concentration [Cmax] was decreased by 61%. When TARCEVA was administered 2 hours following a 300 mg dose of an H-2 receptor antagonist (ranitidine), the erlotinib AUC was reduced by 33% and the erlotinib Cmax was reduced by 54%. When TARCEVA was administered with ranitidine 150 mg twice daily (at least 10 h after the previous ranitidine evening dose and 2 h before the ranitidine morning dose), the erlotinib AUC was decreased by 15% and the erlotinib Cmax was decreased by 17% [see Dose Modifications (2.4), Drug Interactions (7)].
13. Nonclinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Two-year carcinogenicity studies were conducted in mice and rats with erlotinib at oral doses of up to 60 mg/kg/day in mice, 5 mg/kg/day in female rats, and 10 mg/kg/day in male rats. The studies were negative for carcinogenic findings. Exposure in mice at the highest dose tested was approximately 10 times the exposure in humans at the erlotinib dose of 150 mg/day. The highest dose evaluated in male rats resulted in exposures that were twice those in humans and exposures at the highest tested dose in female rats were slightly lower than those in humans.
Erlotinib did not cause genetic damage in a series of in vitro assays (bacterial mutation, human lymphocyte chromosome aberration and mammalian cell mutation) and in the in vivo mouse bone marrow micronucleus test.
Erlotinib did not impair fertility in either male or female rats.
14. Clinical Studies
14.1 Non-Small Cell Lung Cancer (NSCLC) – First-Line Treatment of Patients with EGFR Mutations
Study 1
The safety and efficacy of TARCEVA as monotherapy for the first-line treatment of patients with metastatic NSCLC containing EGFR exon 19 deletions or exon 21 (L858R) substitution mutations was demonstrated in Study 1, a randomized, open-label, clinical trial conducted in Europe. One hundred seventy-four (174) White patients were randomized 1:1 to receive erlotinib 150 mg once daily until disease progression (n = 86) or four cycles of a standard platinum-based doublet chemotherapy (n = 88); standard chemotherapy regimens were cisplatin plus gemcitabine, cisplatin plus docetaxel, carboplatin plus gemcitabine, and carboplatin plus docetaxel. The main efficacy outcome measure was progression-free survival (PFS) as assessed by the investigator. Randomization was stratified by EGFR mutation (exon 19 deletion or exon 21 (L858R) substitution) and Eastern Cooperative Oncology Group Performance Status (ECOG PS) (0 vs. 1 vs. 2). EGFR mutation status for screening and enrollment of patients was determined by a clinical trials assay (CTA). Tumor samples from 134 patients (69 patients from the erlotinib arm and 65 patients from the chemotherapy arm) were tested retrospectively by the FDA-approved companion diagnostic, cobas® EGFR Mutation Test.
Baseline demographics of the overall study population were: female (72%), White (99%), age ≥ 65 years (51%), ECOG PS 1 (53%), with ECOG PS 0 (33%), and ECOG PS 2 (14%), current smoker (11%), past-smoker (20%), and never smoker (69%). The disease characteristics were 93% Stage IV and 7% Stage IIIb with pleural effusion as classified by the American Joint Commission on Cancer (AJCC, 6th edition), 93% adenocarcinoma, 66% exon 19 mutation deletions and 34% exon 21 (L858R) point mutation by CTA.
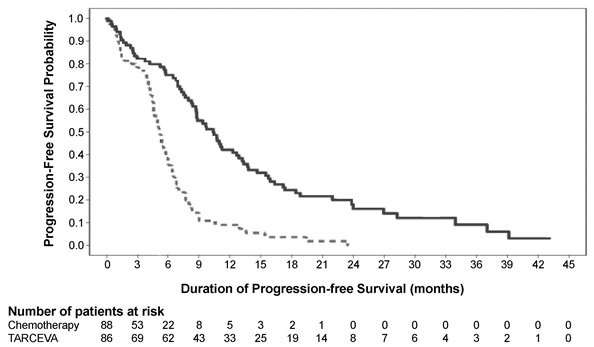
A statistically significant improvement in investigator-determined PFS (based on RECIST 1.0 or clinical progression) was demonstrated for patients randomized to erlotinib compared to those randomized to chemotherapy (see Table 6 and Figure 1). Similar results for PFS (based on RECIST 1.0) were observed for the subgroup evaluated by an independent-review committee (approximately 75% of patients evaluated in Study 1) and in the subgroup of 134 patients (77% of Study 1 population) with EGFR mutations confirmed by the cobas® EGFR Mutation Test.
A protocol-specified analysis of overall survival (OS) conducted at the time of the final analysis of PFS showed no statistically significant difference between the TARCEVA and chemotherapy arms. At the time of the data cut-off, 84% of patients in the chemotherapy arm had received at least one subsequent treatment, of whom 97% received an EGFR-tyrosine kinase inhibitor. In the TARCEVA arm, 66% of patients had received at least one subsequent treatment.
|
||
|
Efficacy Parameter |
Erlotinib
|
Chemotherapy
|
|
Progression-Free Survival |
||
|
Number of Progressions or Deaths |
71 (83%) |
63 (72%) |
|
Median PFS in Months (95% CI) |
10.4 (8.7, 12.9) |
5.2 (4.6, 6.0) |
|
Hazard Ratio (95% CI) * |
0.34 (0.23, 0.49) |
|
|
p-value (unstratified log-rank test) |
< 0.001 |
|
|
Overall Survival |
||
|
Number of Deaths (%) |
55 (64%) |
54 (61%) |
|
Median OS in Months (95% CI) |
22.9 (17.0, 26.8) |
19.5 (17.3, 28.4) |
|
Hazard Ratio (95% CI)* |
0.93 (0.64, 1.35) |
|
|
Objective Response |
||
|
Objective Response Rate (95% CI) |
65% (54.1%, 75.1%) |
16% (9.0%, 25.3%) |
In exploratory subgroup analyses based on EGFR mutation subtype, the hazard ratio (HR) for PFS was 0.27 (95% CI 0.17 to 0.43) in patients with exon 19 deletions and 0.52 (95% CI 0.29 to 0.95) in patients with exon 21 (L858R) substitution. The HR for OS was 0.94 (95% CI 0.57 to 1.54) in the exon 19 deletion subgroup and 0.99 (95% CI 0.56 to 1.76) in the exon 21 (L858R) substitution subgroup.
14.2 NSCLC – Lack of Efficacy of TARCEVA in Maintenance Treatment of Patients without EGFR Mutations
Lack of efficacy of TARCEVA for the maintenance treatment of patients with NSCLC without EGFR activating mutations was demonstrated in Study 2. Study 2 was a multicenter, placebo-controlled, randomized trial of 643 patients with advanced NSCLC without an EGFR exon 19 deletion or exon 21 L858R mutation who had not experienced disease progression after four cycles of platinum-based chemotherapy. Patients were randomized 1:1 to receive TARCEVA 150 mg or placebo orally once daily (322 TARCEVA, 321 placebo) until disease progression or unacceptable toxicity. Following progression on initial therapy, patients were eligible to enter an open-label phase. Baseline characteristics were as follows: median age 61 years (35% age ≥ 65 years), 75% male, 77% White, 21% Asian, 28% ECOG PS 0, 72% ECOG PS 1, 16% never smokers, 58% current smokers, 57% adenocarcinoma, 35% squamous cell carcinoma, 22% stage IIIB disease not amenable to combined modality treatment, and 78% stage IV disease. Fifty percent of patients randomized to TARCEVA entered the open-label phase and received chemotherapy, while 77% of patients randomized to placebo entered the open-label phase and received TARCEVA.
The main efficacy outcome was overall survival (OS). Median OS was 9.7 months in the TARCEVA arm and 9.5 months in the placebo arm; the hazard ratio for OS was 1.02 (95% CI 0.85, 1.22). Median PFS was 3.0 months in the TARCEVA arm and 2.8 months in the placebo arm; the hazard ratio for PFS was 0.94 (95% CI 0.80, 1.11).
14.3 NSCLC – Maintenance Treatment or Second/Third Line Treatment
Two randomized, double-blind, placebo-controlled trials, Studies 3 and 4, examined the efficacy and safety of TARCEVA administered to patients with metastatic NSCLC as maintenance therapy after initial treatment with chemotherapy (Study 3) or with disease progression following initial treatment with chemotherapy (Study 4). Determination of EGFR mutation status was not required for enrollment.
Study 3
The efficacy and safety of TARCEVA as maintenance treatment of NSCLC were demonstrated in Study 3, a randomized, double-blind, placebo-controlled trial conducted in 26 countries, in 889 patients with metastatic NSCLC whose disease did not progress during first-line platinum-based chemotherapy. Patients were randomized 1:1 to receive TARCEVA 150 mg or placebo orally once daily (438 TARCEVA, 451 placebo) until disease progression or unacceptable toxicity. The primary objective of the study was to determine if the administration of TARCEVA after standard platinum-based chemotherapy in the treatment of NSCLC resulted in improved progression-free survival (PFS) when compared with placebo, in all patients or in patients with EGFR immunohistochemistry (IHC) positive tumors.
Baseline demographics of the overall study population were as follows: male (74%), age < 65 years (66%), ECOG PS 1 (69%), ECOG PS 0 (31%), white (84%), Asian (15%), current smoker (55%), past-smoker (27%), and never smoker (17%). Disease characteristics were as follows: Stage IV (75%), Stage IIIb with effusion (25%) as classified by AJCC (6th edition) with histologic subtypes of adenocarcinoma including bronchioalveolar (45%), squamous (40%) and large cell (5%); and EGFR IHC positive (70%), negative (14%), indeterminate (4%), and missing (12%).
|
Efficacy Parameter |
TARCEVA (N = 438) |
Placebo (N = 451) |
|
Progression-Free Survival (PFS) based on investigator assessment |
||
|
Number of Progression or Deaths (%) |
349 (80%) |
400 (89%) |
|
Median PFS in Months (95% CI) |
2.8 (2.8, 3.1) |
2.6 (1.9, 2.7) |
|
Hazard Ratio (95% CI) † |
0.71 (0.62, 0.82) |
|
|
p < 0.0001 |
||
|
Overall Survival (OS) |
||
|
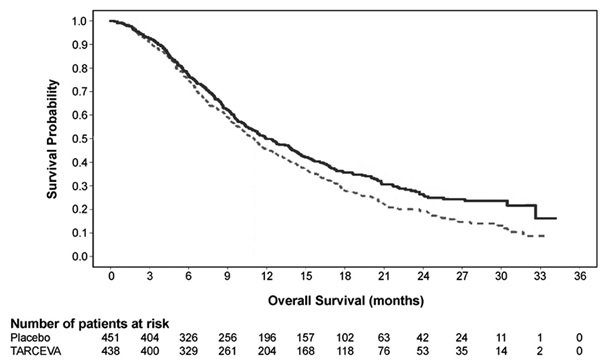
Number of Deaths |
298 (68%) |
350 (78%) |
|
Median OS in Months (95% CI) |
12.0 (10.6, 13.9) |
11.0 (9.9, 12.1) |
|
Hazard Ratio (95% CI) † |
0.81 (0.70, 0.95) |
|
|
p-value (stratified log-rank test) ‡ |
0.0088 |
|
Figure 2 depicts the Kaplan-Meier Curves for Overall Survival (ITT Population).
Note: HR is from a univariate Cox regression model.
Study 4
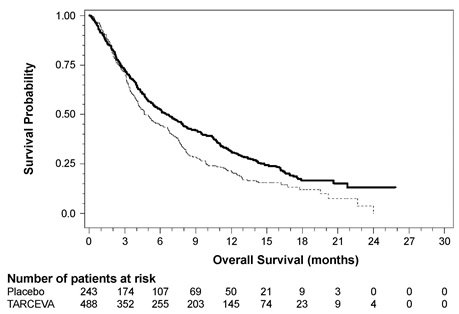
The efficacy and safety of single-agent TARCEVA was assessed in Study 4, a randomized, double blind, placebo-controlled trial in 731 patients with locally advanced or metastatic NSCLC after failure of at least one chemotherapy regimen. Patients were randomized 2:1 to receive TARCEVA 150 mg or placebo (488 TARCEVA, 243 placebo) orally once daily until disease progression or unacceptable toxicity. Efficacy outcome measures included overall survival, response rate, and progression-free survival (PFS). Duration of response was also examined. The primary endpoint was survival. The study was conducted in 17 countries.
Baseline demographics of the overall study population were as follows: male (65%), White (78%), Asian (12%), Black (4%), age < 65 years (62%), ECOG PS 1 (53%), ECOG PS 0 (13%), ECOG PS 2 (25%), ECOG PS 3 (9%), current or ex-smoker (75%), never smoker (20%), and exposure to prior platinum therapy (93%). Tumor characteristics were as follows: adenocarcinoma (50%), squamous (30%), undifferentiated large cell (9%), and mixed non-small cell (2%).
The results of the study are shown in Table 8.
|
||
|
Efficacy Parameter |
TARCEVA (N = 488) |
Placebo (N = 243) |
|
Overall Survival (OS) |
||
|
Number of Deaths |
378 (77%) |
209 (86%) |
|
Median OS in Months (95% CI) |
6.7 (5.5, 7.8) |
4.7 (4.1, 6.3) |
|
Hazard Ratio (95% CI) * |
0.73 (0.61, 0.86) |
|
|
p-value (stratified log-rank test) † |
p < 0.001 |
|
|
Progression-Free Survival (PFS) |
||
|
Number of Progression or Deaths (%) |
402 (82%) |
211 (87%) |
|
Median PFS in Months (95% CI) |
2.3 (1.9, 3.3) |
1.8 (1.8, 1.9) |
|
Hazard Ratio (95% CI)* |
0.59 (0.50, 0.70) |
|
|
Objective Response |
||
|
Objective Response Rate (95% CI) |
8.9% (6.4, 12.0) |
0.9% (0.1, 3.4) |
Figure 3 depicts the Kaplan-Meier curves for overall survival.
14.4 NSCLC – Lack of Efficacy of TARCEVA Administered Concurrently with Chemotherapy
Results from two, multicenter, placebo-controlled, randomized, trials in over 1000 patients conducted in first-line patients with locally advanced or metastatic NSCLC showed no clinical benefit with the concurrent administration of TARCEVA with platinum-based chemotherapy [carboplatin and paclitaxel (TARCEVA, N = 526) or gemcitabine and cisplatin (TARCEVA, N = 580)].
14.5 Pancreatic Cancer - TARCEVA Administered Concurrently with Gemcitabine
The efficacy and safety of TARCEVA in combination with gemcitabine as a first-line treatment was assessed in Study 5, a randomized, double-blind, placebo-controlled trial in 569 patients with locally advanced, unresectable or metastatic pancreatic cancer. Patients were randomized 1:1 to receive TARCEVA (100 mg or 150 mg) or placebo once daily on a continuous schedule plus gemcitabine by intravenous infusion (1000 mg/m2, Cycle 1 - Days 1, 8, 15, 22, 29, 36 and 43 of an 8-week cycle; Cycle 2 and subsequent cycles - Days 1, 8 and 15 of a 4-week cycle [the approved dose and schedule for pancreatic cancer, see the gemcitabine package insert]). TARCEVA or placebo was taken orally once daily until disease progression or unacceptable toxicity. The primary endpoint was survival. Secondary endpoints included response rate, and progression-free survival (PFS). Duration of response was also examined. The study was conducted in 18 countries. A total of 285 patients were randomized to receive gemcitabine plus TARCEVA (261 patients in the 100 mg cohort and 24 patients in the 150 mg cohort) and 284 patients were randomized to receive gemcitabine plus placebo (260 patients in the 100 mg cohort and 24 patients in the 150 mg cohort). Too few patients were treated in the 150 mg cohort to draw conclusions.
In the 100 mg cohort, baseline demographics of the overall study population were as follows: male (52%), white (88%), Asian (7%), black (2%), age < 65 years (53%), ECOG PS 1 (51%), ECOG PS 0 (32%), and ECOG PS 2 (17%). There was a slightly larger proportion of females in the TARCEVA arm (51%) compared with the placebo arm (44%). The median time from initial diagnosis to randomization was approximately 1.0 month. The majority of the patients (76%) had distant metastases at baseline and 24% had locally advanced disease.
The results of the study are shown in Table 9.
|
Efficacy Parameter |
TARCEVA + Gemcitabine (N = 261) |
Placebo + Gemcitabine (N = 260) |
|
Overall Survival (OS) |
||
|
Number of Deaths |
250 |
254 |
|
Median OS in Months (95% CI) |
6.5 (6.0, 7.4) |
6.0 (5.1, 6.7) |
|
Hazard Ratio (95% CI) * |
0.81 (0.68, 0.97) |
|
|
p-value (stratified log-rank test) † |
0.028 |
|
|
Progression-Free Survival (PFS) |
||
|
Number of Progression or Deaths (%) |
225 |
232 |
|
Median PFS in Months (95% CI) |
3.8 (3.6, 4.9) |
3.6 (3.3, 3.8) |
|
Hazard Ratio (95% CI)* |
0.76 (0.64, 0.92) |
|
|
Objective Response |
||
|
Objective Response Rate (95% CI) |
8.6% (5.4, 12.9) |
7.9% (4.8, 12.0) |
Survival was evaluated in the intent-to-treat population. Figure 4 depicts the Kaplan-Meier curves for overall survival in the 100 mg cohort. The primary survival and PFS analyses were two-sided log-rank tests stratified by ECOG performance status and extent of disease.
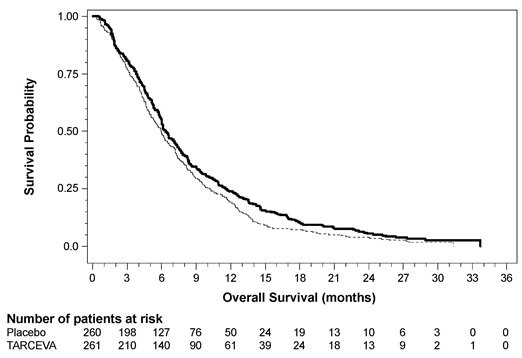
Note: HR is from Cox regression model with the following covariates: ECOG performance status and extent of disease. The p-value is from two-sided Log-Rank test stratified by ECOG performance status and extent of disease.
16. How is Tarceva supplied
25 mg Tablets: round, biconvex face and straight sides, white film-coated, printed in orange with a “T” and “25” on one side and plain on the other side; supplied in:
Bottles of 30: NDC 50242-062-01
100 mg Tablets: round, biconvex face and straight sides, white film-coated, printed in gray with “T” and “100” on one side and plain on the other side; supplied in:
Bottles of 30: NDC 50242-063-01
150 mg Tablets: round, biconvex face and straight sides, white film-coated, printed in maroon with “T” and “150” on one side and plain on the other side; supplied in:
Bottles of 30: NDC 50242-064-01
Store at 25°C (77°F); excursions permitted to 15°C - 30°C (59°F - 86°F). See USP Controlled Room Temperature.
17. Patient Counseling Information
Skin rash, bullous and exfoliative skin disorders
- •
- Advise patients that skin reactions can occur or worsen on sun-exposed areas while taking TARCEVA, and proactive intervention may include alcohol-free emollient cream and use of sunscreen or avoidance of sun exposure. Advise patients that hyperpigmentation or dry skin, with or without digital skin fissures, have been reported and in the majority of cases were associated with rash [see Adverse Reactions (6.1)].
- •
- Advise patients that TARCEVA can increase the risk of bullous and exfoliative skin disorders and to seek immediately medical attention for severe skin reactions [see Warnings and Precautions (5.5)].
Diarrhea
Advise patients that diarrhea can usually be managed with loperamide and to contact their healthcare provider for severe or persistent diarrhea [see Adverse Reactions (6.1)].
Interstitial lung disease
Advise patients of the risk of severe or fatal ILD, including pneumonitis. Advise patients to contact their healthcare provider immediately to report new of worsening unexplained shortness of breath or coughing [see Dosage and Administration (2.4) and Warnings and Precautions (5.1)].
Renal failure
Advise patients of the risk of developing renal failure. Inform patients of the need for the healthcare provider to monitor kidney function and electrolytes [see Warnings and Precautions (5.2)].
Hepatotoxicity
Advise patients to immediately report signs or symptoms of hepatotoxicity [see Warnings and Precautions (5.3)].
Gastrointestinal perforations
Advise patients that TARCEVA can increase the risk of gastrointestinal perforation or fistula and to seek immediate medical attention for severe abdominal pain [see Dosage and Administration (2.4) and Warnings and Precautions (5.4)].
Cerebrovascular accident
Advise patients of the risk of cerebrovascular accident and see immediate medical attention [see Dosage and Administration (2.4) and Warnings and Precautions (5.6)].
Ocular disorders
Advise patients promptly to contact their healthcare provider if they develop eye signs or symptoms, lacrimation, light sensitivity, blurred vision, eye pain, red eye, or changes in vision [see Dosage and Administration (2.4) and Warnings and Precautions (5.8)].
Hemorrhage in patients taking warfarin
Advise patients who are receiving warfarin of the need to monitor INR or other coumarin-derivative anticoagulants [see Warnings and Precautions (5.9) and Drug Interactions (7)].
Hair and nail disorders
Advise patients that hair and nail disorders, including hirsutism and brittle and loose nails, have been reported [see Adverse Reactions (6.1)].
Embryo-fetal toxicity
- •
- Advise pregnant women and females of reproductive potential of the potential risk to a fetus. Advise females of reproductive potential to inform their healthcare provider of a known or suspected pregnancy [see Warnings and Precautions (5.10), Use in Specific Populations (8.1)].
- •
- Advise females of reproductive potential to use effective contraception during treatment with TARCEVA, and for 1 month after the last dose [see Use in Specific Populations (8.3)].
Lactation
- •
- Advise women not to breastfeed during treatment with TARCEVA and for 2 weeks after the final dose [see Use in Specific Populations (8.2)].
Smoking
- •
- Advise patients to contact their health care provider for any changes in smoking status and that the dose of TARCEVA may need to be adjusted if they smoke [see Drug Interactions (7) and Clinical Pharmacology (12.3)]
- •
- Advise patients to stop smoking [see Clinical Pharmacology (12.3)].
Manufactured for:
OSI Pharmaceuticals, LLC, Northbrook, IL 60062
an affiliate of Astellas Pharma US, Inc.
Product of Japan or Italy – See bottle label for origin
Distributed by:
Genentech USA, Inc., A Member of the Roche Group, 1 DNA Way, South San Francisco, CA 94080-4990
For further information please call 1-877-TARCEVA (1-877-827-2382).

TARCEVA® is a registered trademark of OSI Pharmaceuticals, LLC. Other trademarks listed belong to their respective owners.
©2016 Astellas Pharma US, Inc., and Genentech, Inc. All rights reserved.
15J080-TAR-SPL
PRINCIPAL DISPLAY PANEL – 25 mg

NDC 50242-062-01
Tarceva®
(erlotinib)
Tablets
25 mg
Each tablet contains 25 mg of erlotinib free base.
30 Tablets
Rx only
| TARCEVA
erlotinib hydrochloride tablet |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| TARCEVA
erlotinib hydrochloride tablet |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| TARCEVA
erlotinib hydrochloride tablet |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| Labeler - Genentech, Inc. (080129000) |
Frequently asked questions
More about Tarceva (erlotinib)
- Check interactions
- Compare alternatives
- Reviews (42)
- Drug images
- Side effects
- Dosage information
- During pregnancy
- Generic availability
- FDA approval history
- Drug class: EGFR inhibitors
- Breastfeeding